Cases & stories
Patient stories
From Tracey, who had a hip replacement:
‘From first meeting Professor Board, I was really pleased with how we did the whole diagnosis. He was really good all throughout the process. I highly recommend him.’
From L, who had bilateral hip replacements:


‘Dear Tim,
Just thought I’d send you an update. I went skiing for the first time since having my hips done.
You may not recall, however, I was a keen skier before and I used to manage to get out to the alps for 3-4 weeks each season.
We had a lovely time - no off piste anymore… and I still don’t like ice, but the restaurants have lovely views and great seats for people-watching whilst I wait for the others to go and do the silly stuff.>
I’m also playing golf twice a week and managing to maintain my hcp - I have had to rebuild my swing as I’d got into all sorts of compensatory habits. We’ve been away on several golf holidays.
I’m walking Max (the dog) 5 days a week - the other 2 I am in work and he goes to daycare. And I’m hill walking again! (only little ones- it’s still a good excuse).
As a consequence of being able to be more active again, I decided to get some work life balance back and resigned from my CD role and am back in General Practice 2 days a week.’
Hip cases
Cemented primary hip replacement
This 71-year-old lady had been complaining of increasing left hip pain for 2 years. The pain was interfering with her ability to maintain her independence. She had previously undergone a right total hip replacement 10 years ago and this was working well. She underwent a cemented left total hip replacement with full recovery of function and quality of life.
Pre-operative X-ray

Post-operative X-ray

Hip Revision Video using a KAR stem
65-year-old man with loosening of a Charnley Elite Plus stem after 8 years in place. The lateral X ray shows that the original stem was put in an extreme antero-posterior position causing thigh pain and femoral erosion posteriorly at the tip. Surgery addresses the socket first then the stem. The socket is reconstructed with impaction grafting and a cemented implant. The stem used is an uncemented titanium fully hydroxyapatite coated implant (KAR stem -made by DePuy)
Uncemented primary hip replacement
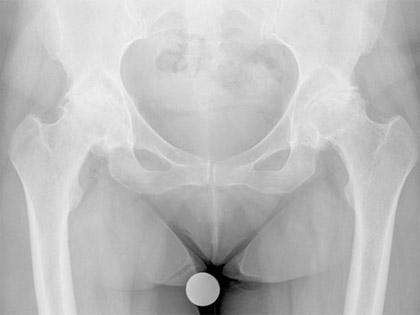
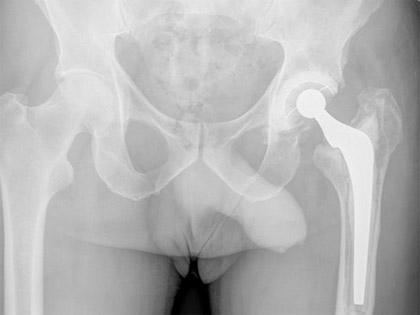
This 43-year-old woman had been suffering with bilateral hip pain for many years. She also had deformities of both hip such that she could not stand up straight and had to stoop forwards. She underwent bilateral (both sides) hip replacement performed on the same day. The prostheses used here are uncemented and the bearing surfaces are ceramic. She was delighted with the outcome of surgery and was able to stand up straight for the first time in years.
Pre-operative X-ray
Post-operative X-ray

Primary hip replacement with impaction bone grafting
This 87-year-old had been wheelchair bound for 9 months prior to surgery. She had severe pain in the hip and the hip was fixed at 70 degrees of flexion. The head of the femur had been completely destroyed and the acetabulum (socket) of the pelvis had been deepened and enlarged with time. The presumed diagnosis was AVN (avascular necrosis). A total hip replacement was performed and chips of allograft(donor) bone were packed into the acetabulum using a technique called impaction grafting to rebuild the bone of the pelvis. A cemented socket and stem were then inserted. She recovered well and left her wheelchair at the hospital.
Pre-operative X-ray

Post-operative X-ray

Primary hip replacement with Structural bone grafting for dysplasia
This 31-year-old lady had undergone multiple previous operations as a child to treat her developmental dysplasia of the left hip. She presented with increasing pain and reduction in the quality of her life due to hip problems. She underwent total hip replacement with a structural bone graft to reconstruct the acetabulum. This can be seen in the post-operative X-ray attached to the pelvis with 2 screws. It was not necessary to remove the previously inserted metal work in the femur
Pre-operative X-ray

Post-operative X-ray

Revision Hip for aseptic loosening of stem and socket
This 65-year-old man developed increasing pin and difficulty weight bearing on his left hip which had been replaced 12 years previously. The X-rays showed loosening of the stem and the socket.
There was no suggestion of infection. The hip was revised using an uncemented stem and impaction grafting with a cemented socket.
Pre-operative X-ray
Post-operative X-ray

Revision hip for peri-prosthetic fracture
This 84-year-old lady had sudden increase in hip pain on the left side after a sight fall. The hip replacement had been loose for some time and the bone had become thin around the implants.
A fracture had occurred in the fall and the hip replacement has clearly subsided in the cement (note the distance between the femoral head and the socket). The hip was revised to a long uncemented stem and the fracture reduced around the stem and held with cerclage wires. The socket was also revised.
Pre-operative X-ray

Post-operative X-ray

Revision hip with impaction grafting to socket and “in-cement�? revision of femur
A 59-year-old gentleman had developed symptoms of pain and feelings of instability in his right hip replacement that had been functioning well for the previous 14 years.
The X-ray shows loosening of the acetabulum (socket). The femoral stem appears well fixed. At revision surgery, the acetabulum was removed easily and reconstruction was undertaken with impaction grafting of a femoral head bone graft followed by cementation of a new socket.
After trial reduction, the hip was found to be unstable so the stem was removed and a new stem with different offset and length was cemented into the old cement mantle, a technique called “in-cement revision”.
Pre-operative X-rays

Post-operative X-ray

Revision hip with structural bone grafting
This 51-year-old lady had three previous revisions of her left total hip replacement. The last one had lasted 10 years when she presented to us with increasing pain and shortening of the leg. The stem was satisfactory but the socket had become loose and migrated proximally.
The hip was revised using a block of allograft(donor) bone, screwed to the pelvis with impaction grafting of more morcellized bone underneath. The socket was then cemented into the new acetabular bed. (oxford score before surgery 48, after surgery 20)
Pre-operative X-ray

Post-operative X-ray

Excision of Heterotopic Ossification from around hip replacement
A 73-year-old gentleman presented with a 5-year history of pain and marked stiffness around his right total hip replacement. His X-rays showed the presences of heterotopic ossification(new bone formation) around the hip joint. This was the cause of the pain and stiffness.
He underwent surgical excision of the bone along with prophylaxis against more HO formations with radiotherapy and indomethacin treatment. His function improved significantly and his pain resolved following surgery.
Pre-operative X-ray

Post-operative X-ray

Femoral osteochondroplasty for hip impingement
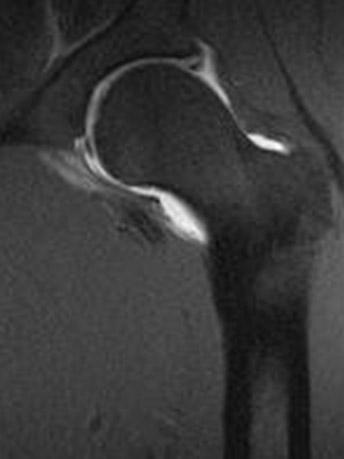
This 40-year-old gentleman presented with pain in the left groin associated with occasional catching sensations which was limiting his activities. Investigations demonstrated classic features of femoro-acetabular impingement(FAI).
The bump on the femoral neck can be clearly seen on the X-rays and CT scan. An MRI arthrogram showed evidence of a labral tear.
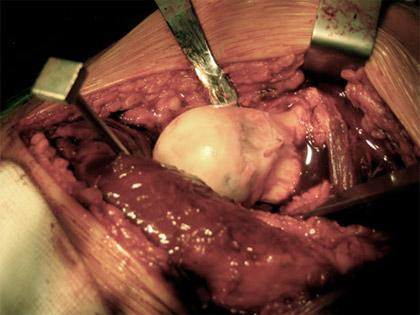
The patient underwent an open hip debridement via a Ganz osteotomy. The neck bump was removed and the labral tear repaired with bone anchors. The patient’s symptoms resolved well following surgery.

Pre-operative X-ray (AP view)

Pre-operative X-ray (Lateral view)

Pre-operative 3D CT scan

Pre-operative MRI Arthrogram showing labral tear
Intra-operative photograph showing bump on femoral neck
Intra-operative photograph showing femoral head-neck junction after osteochondroplasty has been performed

Post-operative X-ray showing anchors in acetabular rim and screws in trochanteric osteotomy
